LondonClinicGuidelines
The London Clinic ICU clinical guidelines repo
Guidelines for Renal Replacement Therapy in the Adult Intensive Care Unit
NOTE: This is a pre-release version and should NOT be used to inform clinical practice until it has been ratified.
Aim
To provide general guidance on the principles and provision of renal replacement therapy in intensive care unit.
Scope
All adult patients in Critical Care.
Version Control
- This document is automatically version controlled by a technology called git.
- Revisions are due:
Contributors
- Dr Niall MacCallum
- Dr Edward Palmer
Other Relevent Documents
This document is to be used in conjunction with:
- Systemic anticoagulation with unfractionated heparin guideline
- Epoprostenol
- Filter set up document
- Thromboprophylaxis guideline
Disclaimer
…
Indications for Renal Replacement Therapy (RRT)
Primary goal of RRT is to compensate for loss of renal function & correct it’s associated sequelae, including:
- Accumulation of nitrogenous waste products
- Electrolyte disturbances
- Metabolic acidosis
- Volume overload
Indications for commencing RRT:
- Development of uraemic signs or symptoms
- Management of fluid overload
- Electrolyte disturbance:
- Hyperkalaemia >6.5 refractory to medical therapy
- Less common: Na, Ca, phosphate , Mg & uric acid
- Metabolic acidosis
- Dialyzable or filterable toxins (Aspirin, Lithium, Methanol, Ethylene Glycol, Methotrexate, Theophylline, myoglobin metabolites etc.)
Types of RRT
Intermittent vs. continuous
Continuous RRT is applied for (or aimed at being applied for) 24 hours/day Advantages: slower fluid removal therefore more haemodynamically stable, the slower control of solute concentration therefore avoiding large fluctuations and fluid shifts Disadvantages: Need for immobilisation, the use of continuous anticoagulation, risk of hypothermia
Intermittent RRT is performed for less than 24 hours in a 24 hour time frame several times per week Advantages: Fast removal of toxins and decreased treatment time Disadvantages: Theoretically causes greater haemodynamic instability with large fluid shifts (risk of cerebral oedema), technically more complex and demanding, expensive
The London Clinic ICU uses continuous RRT
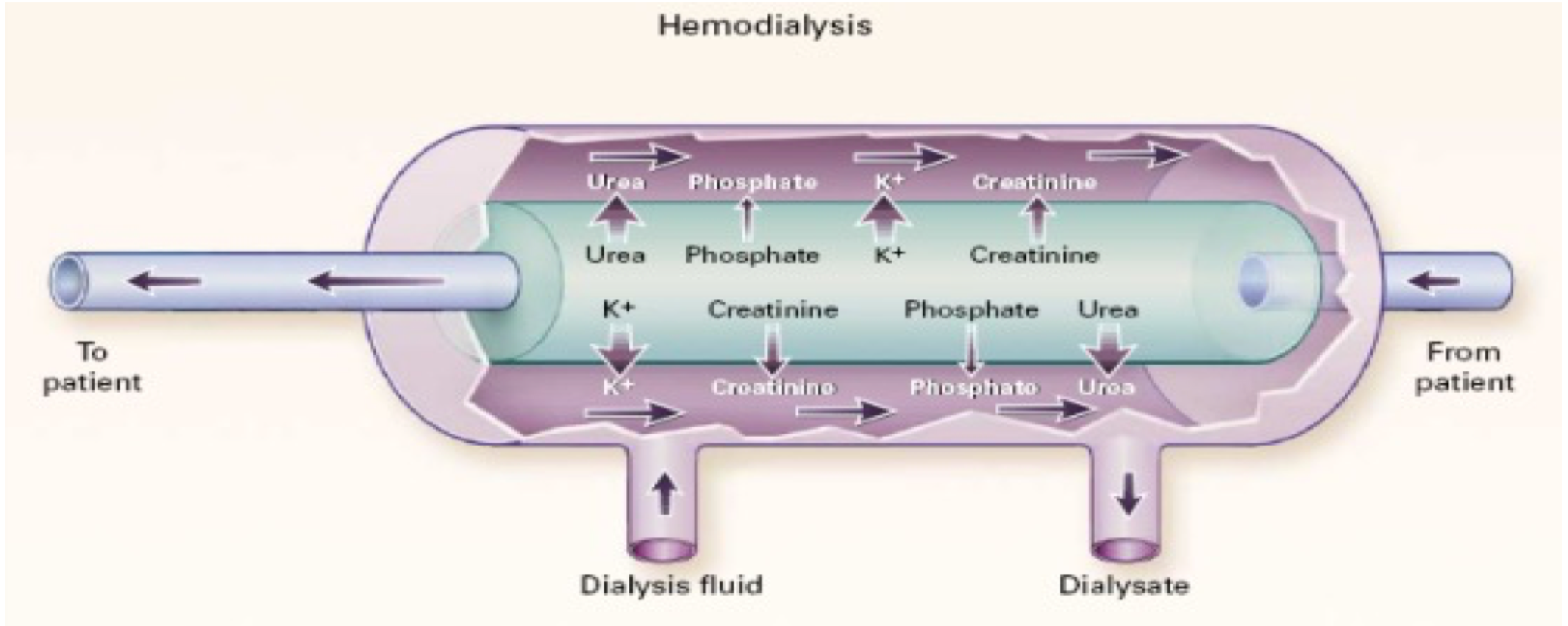
Haemodialysis
The mechanism of solute clearance is by diffusion. Solutes in blood pass down a concentration gradient across a semi-permeable membrane, which is maintained by the counter flow of dialysate replacement fluid.
In Figure 1 below the arrows that cross the membrane indicate the predominant direction of movement of each solute through the membrane; the relative size of the arrows indicates the net amounts of the solute transferred. Other arrows indicate the direction of fluid flow.
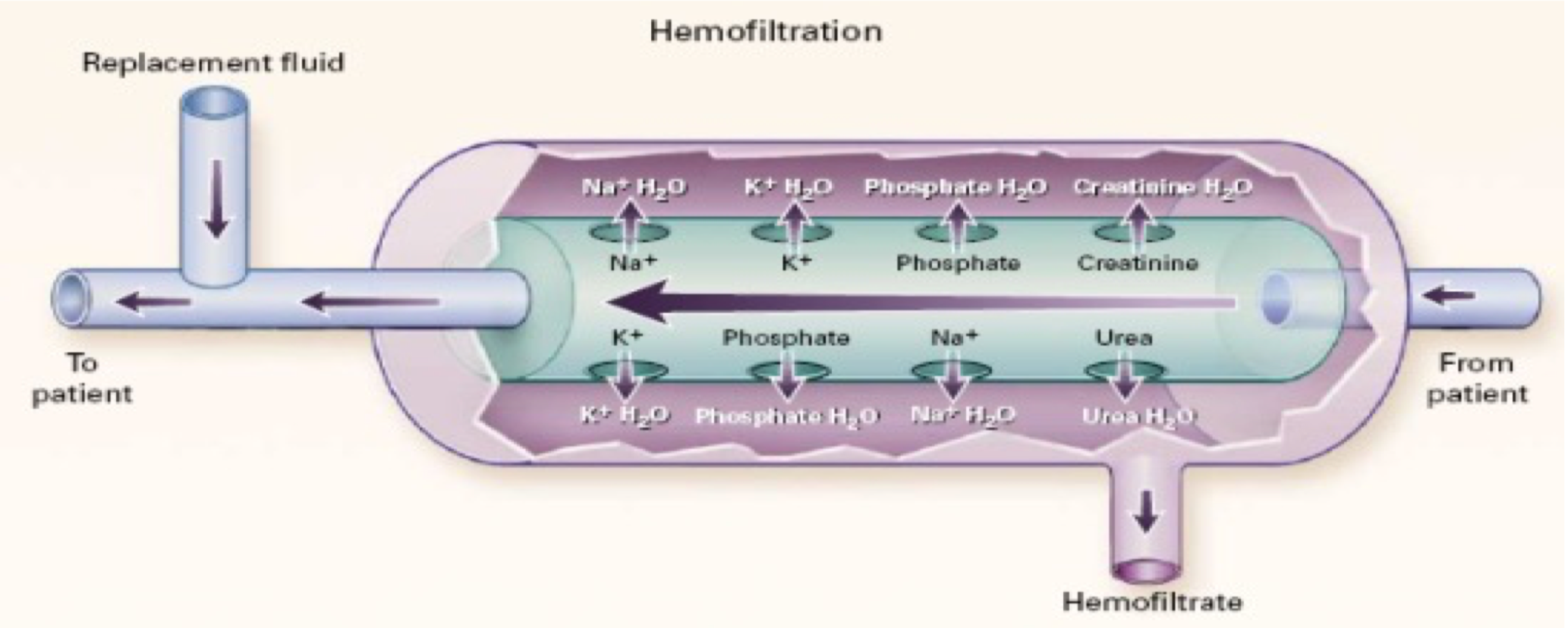
Haemofiltration
The mechanism of solute clearance is by convection. Blood under pressure passes down one side of a highly permeable membrane allowing both water and substances up to molecular weights of between 30-50,000 kDa to pass across the membrane by convective flow. Refer below to Figure 2.
Peritoneal dialysis
Peritoneal dialysis is an alternative mechanism of renal replacement therapy. Fluid is instilled into the abdomen via a special catheter and allowed to remain there for some time (dwell time), during which fluids and electrolytes diffuse across the peritoneal membrane.
This guideline does not consider peritoneal dialysis
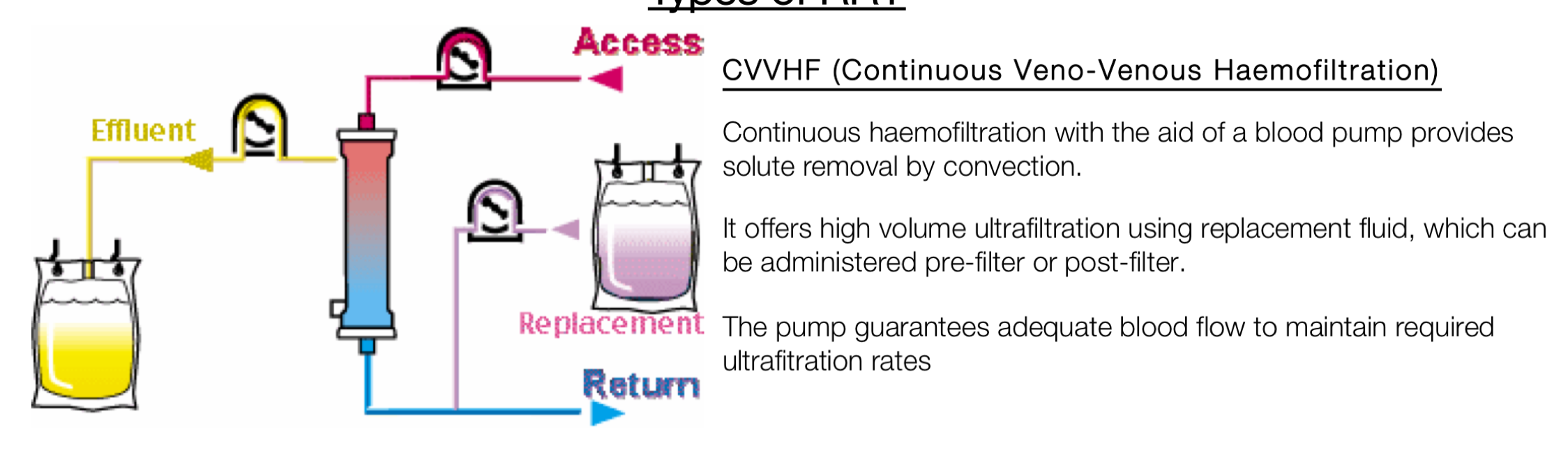
CVVHF
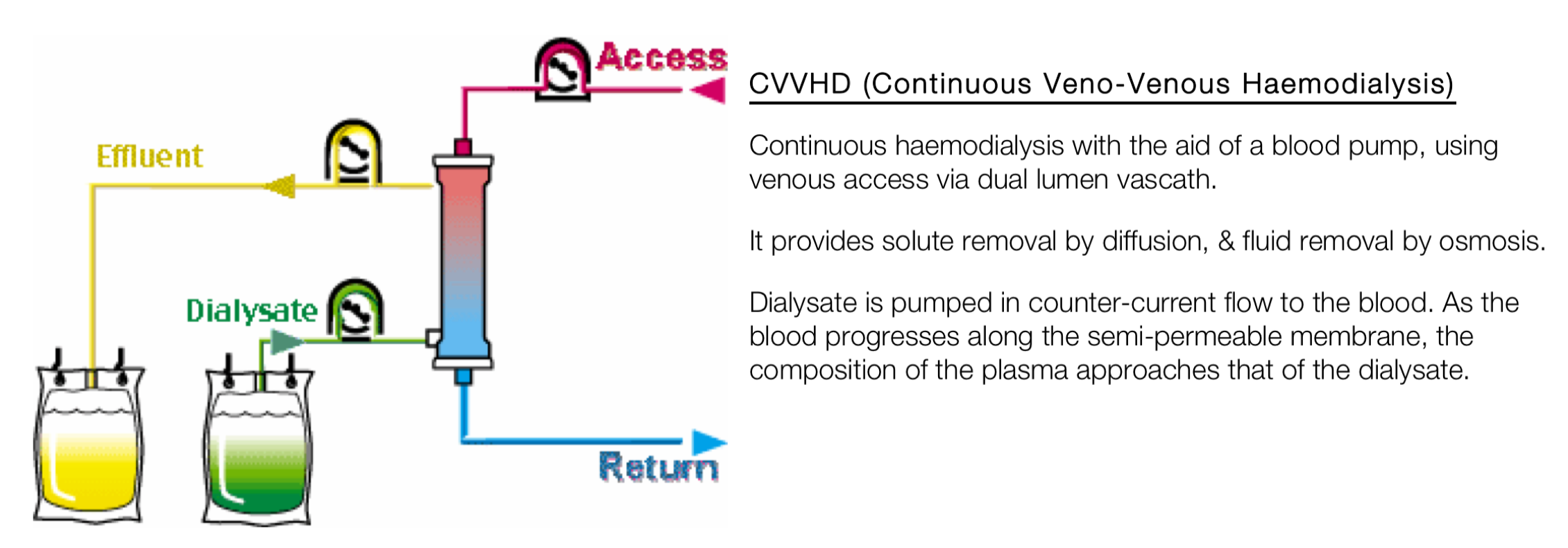
CVVHD
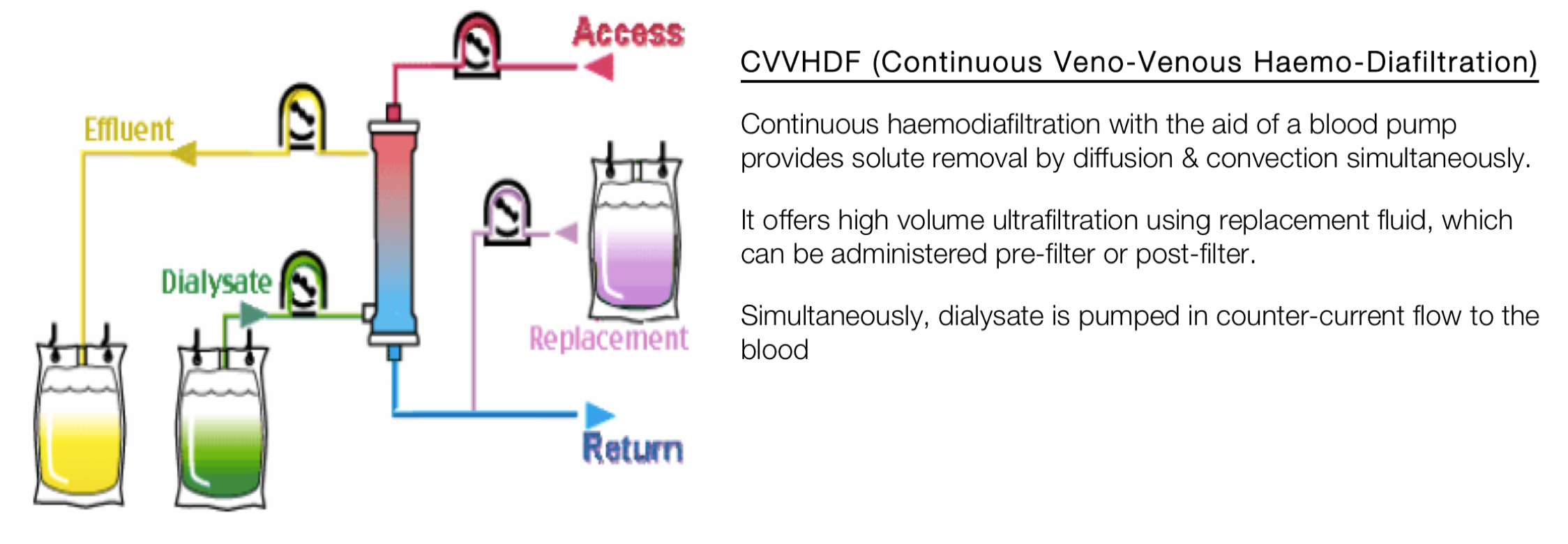
CVVHDF
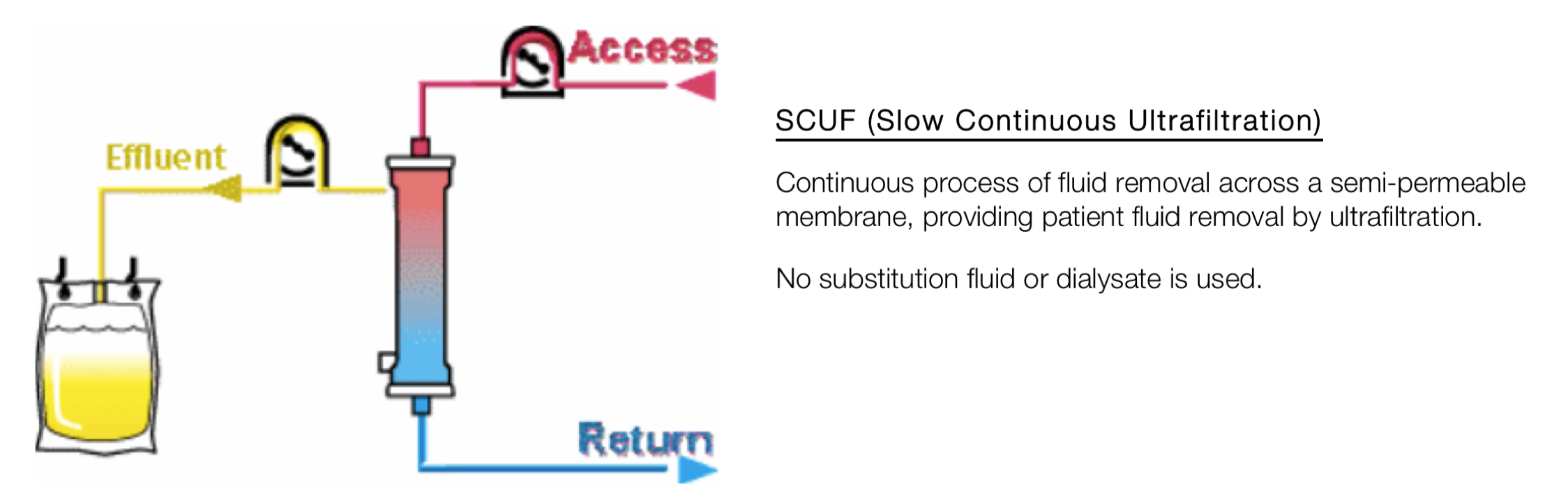
SCUF
Vascular Access
Blood flow through the haemofilter circuit is dependent on good access to the blood stream. The better the flow of blood the more efficient the treatment and the longer the filter lasts. If the pressures in the circuit become too great (i.e too negative in venous arm and too positive across the membrane or in the arterial arm) then the machine will alarm, the blood pump stops and the chance of clotting the circuit increases. Micro-bubbles can also form in the circuit if the negative pressure in the venous arm is too great.
Correct type and placement of the venous dialysis catheter is essential to maintain good flow.
Type of catheter:
- MAHURKAR 11.5Fr x 16 cm for internal jugular or subclavian
- MAHURKAR 19.5 cm line equivalent for femoral
Insertion Site: First choice: Internal jugular vein (right in preference to the left) Exception: Femoral vein to be used first line in the following situations:
- Emergencies
- Significant coagulopathies
- Un-intubated patients unable to lie flat
- Access problems causing filter clotting
- Definite plan for high-flux haemofiltration
Subclavian veins are less favoured due to flow problems and the increased incidence of stenosis which has implications for long term renal support or permanent pacing. Contraindicated in coagulopathic patients
All lines must be inserted under ultrasound guidance using full aseptic technique
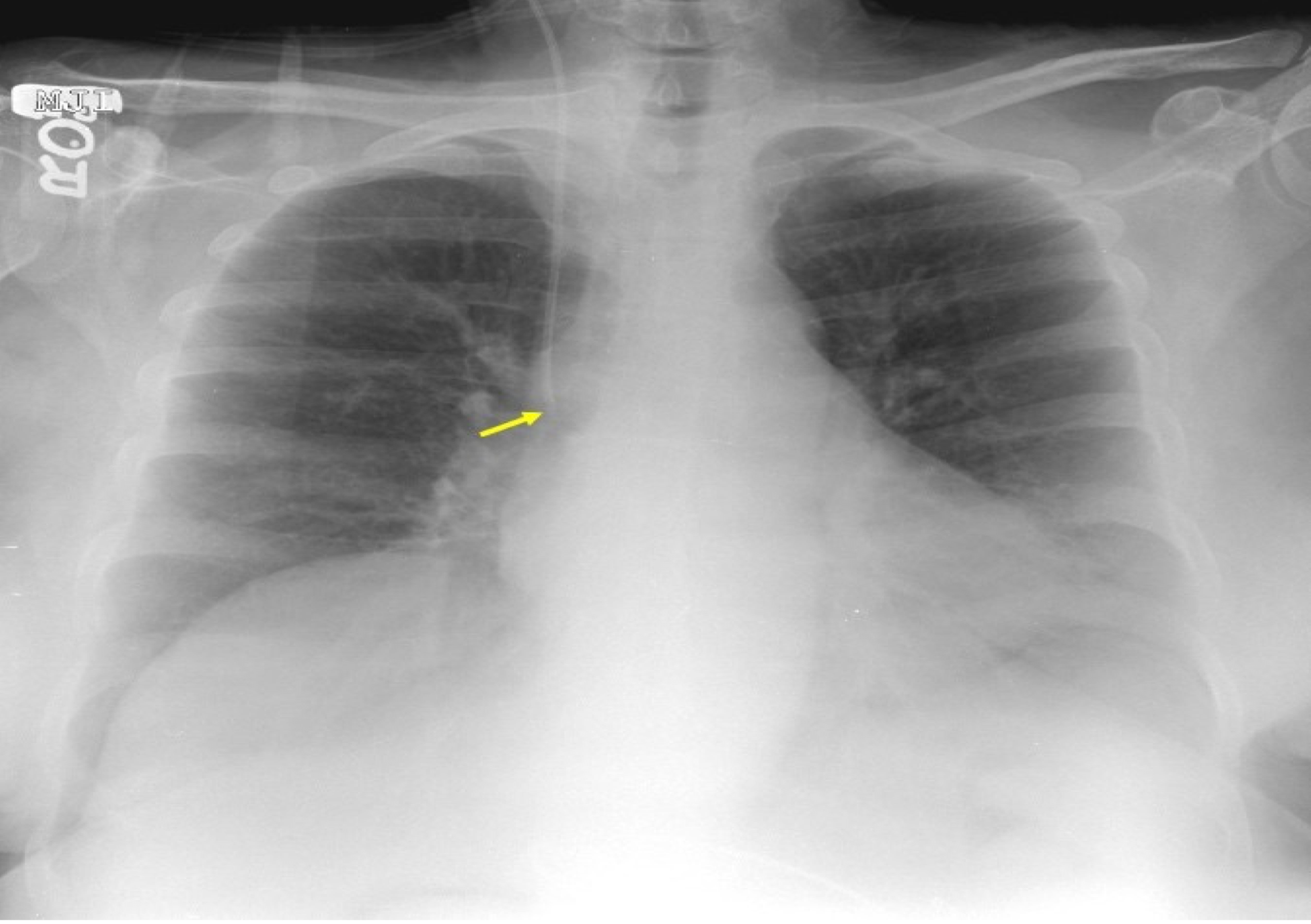
Placement: The optimal position for the tip of a dialysis catheter (when inserting via the internal jugular or subclavian vein) is in the region of the superior vena cava – right atrial junction, typically at the level of the right main bronchus (see below)
Catheter Lock – Heparin Lock
Vascular access may become compromised with clot if an anticoagulant agent is not locked within the catheter lumens. All dialysis catheters should be heparin locked (add heparin concentrate) access if not in use for more than 4 hours (unless heparin is contraindicated e.g. patient has HIT).
Heparin-lock MUST be ASPIRATED prior to re-using the lines
| Catheter type | Proximal lumen (red) | Distal lumen (blue) |
|---|---|---|
| MAHURKAR 11.5Fr x 16 cm | ? | ? |
| MAHURKAR 11.5Fr x 19.5 cm | ? | ? |
Approach to Anticoagulation for RRT
Systemic unfractionated heparin:
- CVVHF 1L exchange unless otherwise stated by ICU consultant
- Systemic heparin administration (given pre-filter) as per ICU guidance (link to guidance).
- Aiming for APPTR: 2 – 2.5
- All patients on systemic heparin should be monitored for Heparin Induced Thrombocytopaenia (HIT), if HIT is suspected the patient should be discussed with the haematology anticoagulation team.
Epoprostenol / Prostacyclin (PGI2):
- CVVHF 1L exchange unless otherwise stated by ITU consultant
- Prostacyclin may be used in cases of HIT or in some patients with hepatic failure where heparin has little anticoagulant effect due to low antithrombin III levels and frequent clotting is problematic
- Prostacyclin may be administered in conjunction with heparin or as a sole therapy
- Epoprostenol / Prostacyclin and Heparin can be administered together (by 3 way tap) into the predilution anticoagulation line of both the Infomed and Prismaflex machines
- Refer to the guidance for Epoprostenol (link)
Thromboprophylaxis during RRT
Thromboprophylaxis should be administered according to the hospital guidelines for all patients during RRT (unless the patient is being systemically anticoagulated with unfractionated heparin for RRT or other has other contraindications to thromboprophylaxis).
Graduated compression stockings and/or intermittent pneumatic compression devices should be used unless contraindicated
Haemodynamically unstable patients
Commencement of haemofiltration can cause cardiovascular instability. Consider the following:
- Prepare metaraminol (10mg in 20mL) before initiation of therapy
- Prepare a colloid infusion that can flow rapidly before initiation of therapy
- Start with a blood flow rate 50mL/min and titrate up as tolerated to the target blood flow rate
Anticipate falls in blood pressure with small doses of metaraminol, rather than attempting to rescue severe hypotension
PRISMAFLEX Haemofiltration with Heparin or Epoprostenol Anticoagulation
- Collect all relevant equipment:
- filter set
- effluent bags
- 2 x 1000mls 0.9% Sodium Chloride
- 5000 units heparin (for priming)
- 20,000 units heparin OR Epoprostenol for infusion as per prescription
- In the setting up therapy screen always choose CVVHDF regardless if you plan to use CVVH or CVVHDF (This will enable you to change from CVVH to CVVHDF if you need to during therapy and avoid restarting a whole new set).
- In the anticoagulant screen always choose ‘No anticoagulation’ (Although you may be using Heparin or Epoprostenol we will not be using the integral syringe pump on the Prisma machine, and will instead use a separate BBraun syringe Driver).
- Prepare 5000 units heparin in the 1st 1000mls bag of 0.9% Sodium Chloride for priming the circuit and have the 2nd 1000mls (without heparin) bag ready for re-priming.
- Continue loading set as you would if you were setting up the Prisma for use with Citrate and confirm set and flow rates. Do not clamp the syringe line (green tip) as we will use this line with the external syringe driver.
- Confirm fluid loss alarm as 400ml - please do not adjust this as is a safety issue. Continue priming process as per screen instructions
| For CVVH therapy | For CVVHDF therapy |
|---|---|
| Pre-dilution scale (white) - Replacement fluid eg Monosol, PrismoSol | Pre-dilution scale (white) - Replacement fluid eg Monosol, PrismoSol |
| Post dilution scale (purple) - Replacement fluid eg Monosol, PrismoSol | Post dilution scale (purple) - Replacement fluid eg Monosol, PrismoSol |
| Dialysate scale (green) - Hang a bag of 1 litre 0.9% normal saline | Dialysate scale (green) - Replacement fluid eg Monosol, PrismoSol |
- Prepare 20000 units Heparin or Epoprostenol infusion as per prescription and remember to record in the infusion section on ICIP.
- Place the infusion in the external syringe driver. Attach syringe and giving set to the syringe line in the filter set (with green anti-syphon tip). When you prime the line of the syringe driver giving set, prime an additional 1ml to ensure the filter line has also been primed. If this is forgotten or you are concerned there is still air in the line, this air will be detected by the aeration chamber.
What rates to set?
Examples: For a 1 litre exchange on CVVH:
- Pre-blood pump set to 500mls
- Replacement set to 500mls
- Dialysate set to 0 mls
- Set fluid removal rate (as per fluid balance target)
For a 2 litre exchange on CVVHDF
- Pump speed aim
- Pre-blood pump set to 500mls
- Replacement set to 500mls
- Dialysate set to 1000mls
- Set fluid removal rate (as per fluid balance target)
Recommended Programming Guide CVVH
| Total Exchange mls/hour | Pre blood pump (PBP) mls/hr | Replacement mls/hr | Min. blood pump speed(mls/min) |
|---|---|---|---|
| 1000 | 500 | 500 | 150 |
| 1500 | 500 | 1000 | 180 |
| 1800 | 600 | 1200 | 200 |
| 2000 | 700 | 1300 | 220 |
| 2300 | 900 | 1400 | 250 |
| 2500 | 1000 | 1500 | 280 |
Recommended Programming Guide CVVHDF
| Total Exchange mls/hr | Pre blood pump (PBP) mls/hr | Replacement mls/hr | Dialysate mls/hr | Min. blood pump speed(mls/min) |
|---|---|---|---|---|
| 1000 | 200 | 300 | 500 | 150 |
| 2000 | 500 | 500 | 1000 | 180 |
| 3000 | 600 | 900 | 1500 | 200 |
- Go to ‘confirm all’ then ‘continue’.
- Now connect the patient as per the screen. At this point the Y connector should be removed (this is what we use when delivering calcium to the return line as part of citrate therapy) and attached directly red to red port and blue to blue port.
- Commence therapy as normal. Remember to start the external syringe driver containing the Heparin or Epoprostenol as per prescription
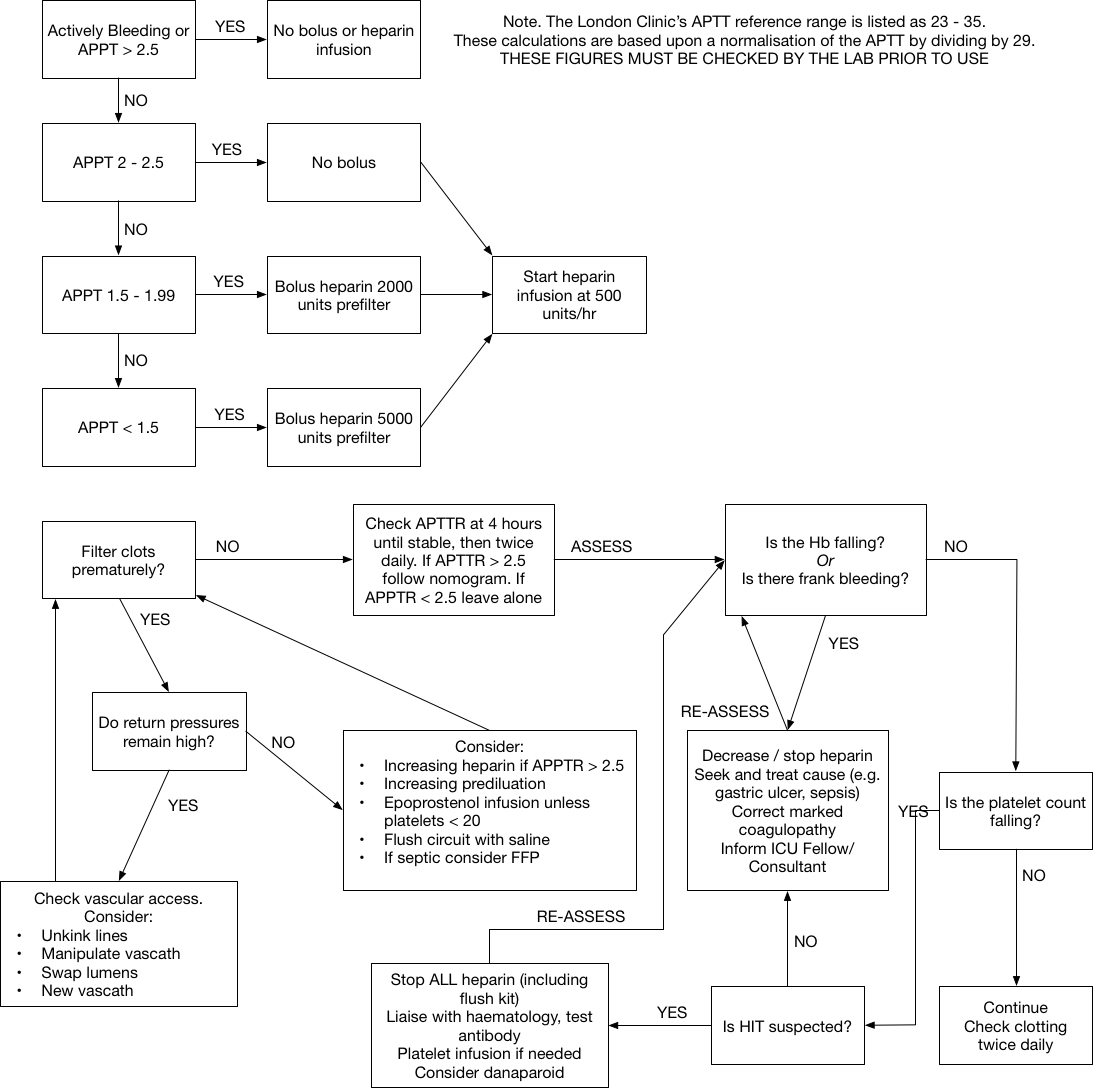
Refer to Figures below regarding management of Heparin and Epoprostenol and/or refer to separate guidelines
Nomogram for Heparin Sodium Infusion for CRRT - concentration 1,000 units/ml
| APTTR | Infusion Rate Change |
|---|---|
| > 6.2 | Stop for 2 hours, reduce by 500 units/hour (0.5 ml/hr), recheck urgently at 4 hours once restarted |
| 4.21 - 6.2 | Stop for 1 hour, reduce by 300 units/hour (0.3 ml/hr), and recheck urgently at 4 hours once restarted |
| 3.61 - 4.2 | Reduce by 200 units hour (0.2 ml/hr), and recheck at 4 hours |
| 2.51 - 3.6 | Reduce by 100 units/hour (0.1 ml/hr) and recheck in 4 hours |
| 1.51 - 2.5 | No change if no signs of filter clotting, recheck APTTR in 6 hours. If filter shows signs of clotting increase by 100 units/hour, consider repeat bolus of 2,000 units heparin, recheck APTT in 6 hours |
| 1 - 1.5 | No change if no signs of filter clotting, recheck APTTR in 6 hours. If filter shows signs of clotting consider bolus of 2,000 units heparin, and increase infusion by 400 units/hour, recheck APTT in 6 hours |
NOTE: The London Clinic’s APTT reference range is listed as 23 - 35. These calculations are based upon a normalisation of the APTT by dividing by 29. THESE FIGURES MUST BE CHECKED BY THE LAB PRIOR TO USE
Send specimens to the lab marked “Urgent - on heparin”
Overnight
It is not always essential to replace a clotted haemofilter between midnight and 08:00. Consider delaying re-initiation of therapy until the morning in patients who have been established on haemofiltration for over 24 hours and who also fulfil the following criteria:
- Serum potassium <6 mmol/L
- pH>7.30
- Projected fluid balance at 08.00 not likely to compromise the patient
- No specific instructions made on the ward round to continue haemofiltration
- Patient is not being cooled for a neurological injury
If haemofiltration is delayed > 4 hours then catheters should be locked with unfractionated heparin
References
- Asquith JR. Dialysis Access Management. In: Cowling MG, ed. Vascular Interventional Radiology: Springer; 2007:125 – 34.
- Brocklehurst IC, Thomas AN, Kishen R, Guy JM. Creatinine and urea clearance during continuous veno-venous haemofiltration in critically ill patients. Anaesthesia 1996;51:551-3.
- Manns M, Sigler MH, Teehan BP. Continuous renal replacement therapies: an update. Am J Kidney Dis 1998;32:185-207.
- Eknoyan G, Beck GJ, Cheung AK, et al. Effect of dialysis dose and membrane flux in maintenance hemodialysis. N Engl J Med 2002;347:2010-9.
- Bellomo R, Cass A, Cole L, et al. Intensity of continuous renal-replacement therapy in critically ill patients. N Engl J Med 2009;361:1627-38.
- Bouman CS, Oudemans-Van Straaten HM, Tijssen JG, Zandstra DF, Kesecioglu J. Effects of early high-volume continuous venovenous hemofiltration on survival and recovery of renal function in intensive care patients with acute renal failure: a prospective, randomized trial. Crit Care Med 2002;30:2205-11.
- Ronco C, Bellomo R, Homel P, et al. Effects of different doses in continuous venovenous haemofiltration on outcomes of acute renal failure: a prospective randomised trial. Lancet 2000;356:26-30.
- Saudan P, Niederberger M, De Seigneux S, et al. Adding a dialysis dose to continuous hemofiltration increases survival in patients with acute renal failure. Kidney Int 2006;70:1312-7.
- Tolwani AJ, Campbell RC, Stofan BS, Lai KR, Oster RA, Wille KM. Standard versus high-dose CVVHDF for ICU-related acute renal failure. J Am Soc Nephrol 2008;19:1233-8. 10. Palevsky PM, Zhang JH, O’Connor TZ, et al. Intensity of renal support in critically ill patients with acute kidney injury. N Engl J Med 2008;359:7-20. 11. KDIGO Clinical Practice Guideline for Acute Kidney Injury, Kidney International Supplements, VOLUME 2, ISSUE 1, MARCH 2012 12. Royal Brompton and Harefield Guidelines for continuous venovenous renal replacement therapy in the Adult Intensive Care Unit 2015, United Kingdom 13. Alfred Health Guidance for Continuous Renal Replacement Therapy in ICU, Melbourne, Australia 13 . Austin Health, Clinical guideline for CRRT in the intensive care unit 2015, Melbourne, Australia
- University College London Hospital ICU Clinical Guidelines for Renal Replacement Therapy. 2018. London, UK.