RENOVATE Trial
Or… an introduction to Bayesian learning

ST8 in Anaesthesia & Intensive Care Medicine
2025-05-23
Learning Objectives / Housekeeping
- Develop an intuition for Bayesian statistics.
- Appreciate the differences between Bayesian and frequentist reasoning.
- Unlearn a few bad statistical habits!
- No maths. No formulas*. Accessible to all.
- Interactive. Feel free to interrupt.
- No singling out, but volunteers welcome.
- Some statistical concepts are so ingrained, keep an open mind.
Let’s Challenge Our Assumptions
- An RCT investigated the effect of steroids in septic shock on mortality.
- Mortality was 43% in the treatment group and 49.1% in the control group (p = 0.03).
- What is the correct interpretation of this p value?
Let’s Challenge Our Assumptions
- An RCT investigated the effect of steroids in septic shock on mortality.
- The relative risk of mortality in the treatment group was 0.88 (95% confidence interval, 0.78 to 0.99).
- What is the correct interpretation of this 95% confidence interval?
My Prediction
- No more will get the answers than would be expected by random chance.
- These are hard questions, but foundational.
- These concepts come from “Frequentist statistics”.
- Bayesian statistics conceptualises probabilities differently.
- Most frequentist statistics are interpreted incorrectly; already Bayesian?
- If you are confused. That’s ok.
Setting
- 33 Brazilian hospitals
- Nov 2019 - Nov 2023
- HFNO vs NIV for ARF
Background
- Number of different approaches to managing ARF
- Pharmacological:
- Bronchodilators
- Antibiotics
- ..
- Oxygen
- Non-pharmacological
- Positioning
- Sputum clearance
- Mechanical support: IMV, NIV/CPAP, HFNO
Background
Non-invasive Ventilation
- Delivers a pressure differential
- Can titrate O2 occording to need
- Augments minute volume
- Applies PEEP
- Limits interventions, often poorly tolerated
- Need breaks to eat etc.
High Flow Nasal Oxygen
- Provides high inspiratory flow in excess of peak inspiratory flow
- Bulk flow reduces deadspace
- Comfortable; patients wear it for longer.
- Heated and humidified
- ?PEEP; skeptical
Background
- Both are useful tools when used correctly.
- Dynamic evidence landscape
- Infective aetiologies and NIV?
- RECOVERY-RS: CPAP
- FLORALI: HFNO
- HERNANDEZ: HFNO
Population
- Inclusion Criteria:
- Aged \(\geq\) 18 y/o admitted to hospital (ED/ICU/Wards) with ARF
- Spo2 <90% or PaO2 < 7.9 kPa RA
- Signs of increased WOB or tachypnoea >25 bpm
Population
- Exclusion Criteria:
- Urgent need for endotracheal intubation
- Prolonged respiratory pauses
- Cardiorespiratory arrest
- GCS \(\leq\) 12
- Heart rate < 50 bpm with decreased level of consciousness
- Arterial blood pH < 7.15
- Haemodynamic instability
- Contraindication to NIV (vomiting, secretions, GCS < 12, pneumothorax)
- Do not intubate order
- NIV use in ACPO prior to randomisation
Population
- Nonimmunocompromised ARF
- Immunocompromised ARF
- Acute Cardiogenic Pulmonary Oedema (ACPO)
- COPD
- COVID-19
Intervention
- HFNO
- Airvo-2, Fisher & Paykel Healthcare
- Flow:
- 30L/min in COPD, 45L/min otherwise
- Titrated up to 60L/min as tolerated
- FiO2:
- Started at 0.5
- COPD: titrated for SpO2 88-92%
- Other groups: 92-98%
NIV rescue therapy was allowed for COPD and ACPO only.
Control
- NIV (face mask)
- Pressure:
- COPD: IPAP 12-16 cmH2O, EPAP 4 cmH2O
- Other groups: IPAP 12-14 cmH2O, EPAP 8cmH2O
- Maximum IPAP 20 cmH2O EPAP of 12cmH2O
- Tidal volume:
- 6-9 ml/Kg* of ideal body weight
- FiO2: as for intervention
- Pressure:
24hr use of NIV encouraged.
Outcome
- Primary: Endotracheal intubation (or death) within 7 days of randomisation
- Criteria for intubation standardised
- Secondary:
- 28 + 90 day mortality
- Mechanical ventilation-free days at 28 days
- ICU-free days at 28 days
- Tertiary:
- ICU + Hospital LOS within 90 days
- Vasopressor-free days within 28 days
- The proportion of patients who received a do-not-intubate order within 7 days after randomisation
Key Methods
Non-inferiority unblinded bayesian adaptive randomised controlled trial.
5 distinct groups.
“Adaptive”; dynamic borrowing.
1:1 randomisation, permuted block size, allocation concealment.
Interim analyses: futility, non-inferiority, or superiority.
Composite outcome.
Key Methods
Non-inferiority unblinded bayesian adaptive randomised controlled trial.
5 distinct groups.
“Adaptive”; dynamic borrowing.
1:1 randomisation, permuted block size, allocation concealment.
Interim analyses: futility, non-inferiority, or superiority.
Composite outcome.
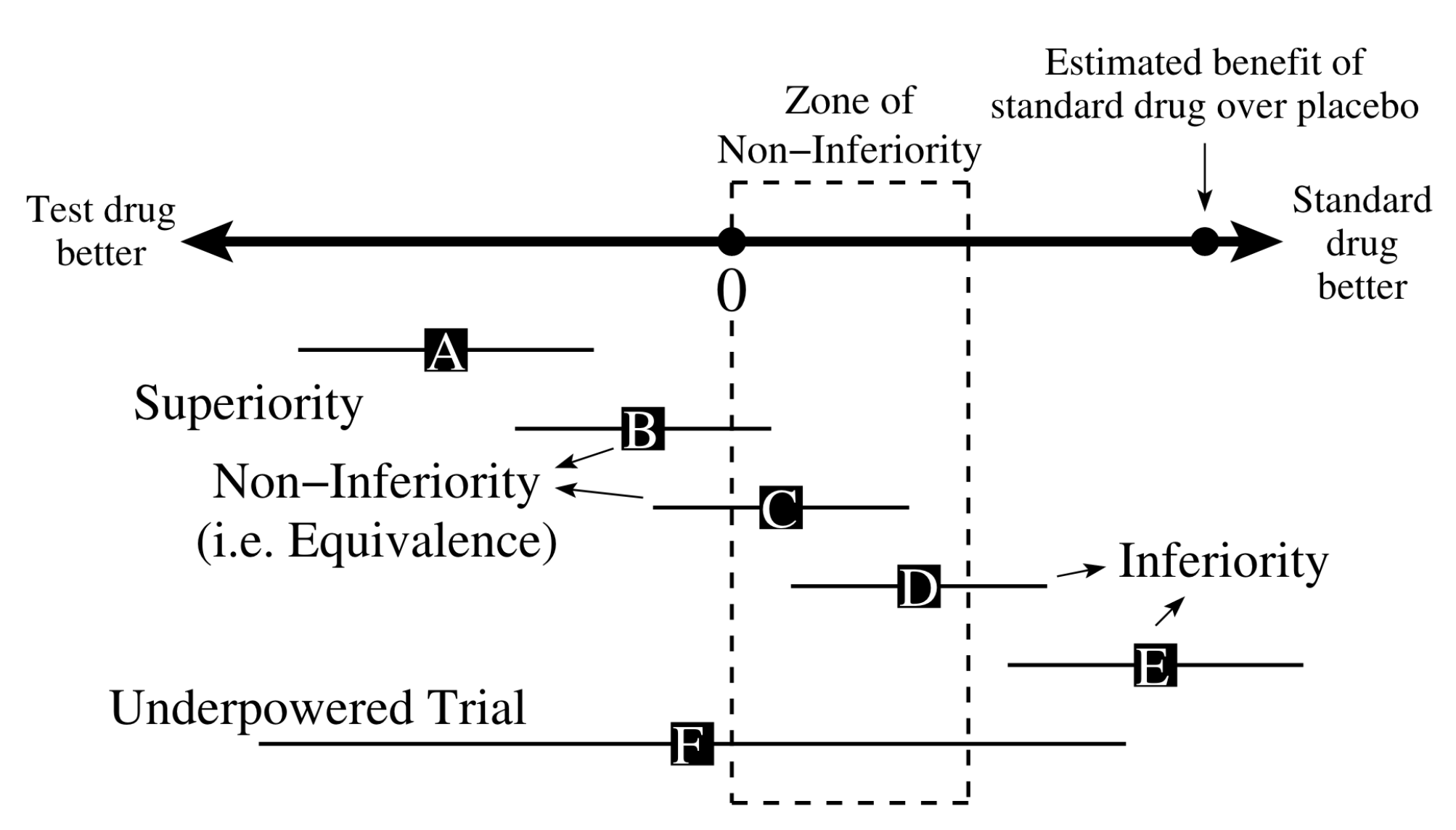
Non-inferiority Trial
- Most RCTs are “superiority” trials; is one treatment “better” than the other?
- Is this always necessary?
- Is one treatment less toxic or less expensive?
- One can be “better” if clinical efficacy the same.
- How do you prove that two treatments are the same?
- Can anyone recognise the issue?

It’s About precision
- Without enough data, all comparisons are non-inferior
Let’s go Bayesian
- A simulated trial
- Population: 10 Adults from the general population admitted to the ICU with a diagnosis of septic shock.
- Intervention: “Vaso-pushin”™; 5 patients
- Control: Standard care; 5 patients
- Outcome: Increase in MAP. MCID increase of 10 mmHg assuming baseline MAP of 55.
Borrowing
- Let’s conduct a thought experiment
- Consider an RCT in ARF conducted in 2024 and another in 2025.
- How might information transfer from one to the other?
- Could we include the controls of the 2024 study as “controls” in the 2025 study?
- Why might we want to do this?
Borrowing
- Bayesian approach naturally allows for borrowing
- Caution must be exercised
- Are the groups really similar? Are they “exchangeable”?
- Increased precision
- But… results will gravitate towards the group mean
Trial Results
Stopping Criteria
- April 2021 (1st interim); immunocompromised. Futility. n = 51
- March 2023 (5th interum); COVID-19, non-inferiority. n = 895
- Oct 2023 (6th interum); Non-immunocomprimise, non-inferiority. n = 501
- Oct 2023 (6th interum); Cardiogenic pulmonary oedema, non-inferiority. n = 274
- Final analyis: COPD. n = 79
Conclusions
Conclusions
- Met pre-specified criteria for non-inferiority for 4 of 5 cohorts
- But… results not robust to strong modelling assumptions (borrowing)
- Need further study: COPD, immunocompromised and ACPO
Stengths
- Large, multi-centred RCT.
- Bayesian; transparent.
- Auhtors conclusions are well made.
- Broad generalisability for the patients I see.
- Others…
Weaknessess
- Late (but necessary) inclusion of COVID-19 to trial protocol.
- Modification of trial protocol to include death as composite outcome.
- Very small numbers for COPD ?selection bias.
- Over/inappropriate borrowing from dissimilar groups; failed sensitivity analysis.
- Criteria for futility too harsh.
- High cross over from HFNO to NIV in COPD.
- Others…
My Take Aways
- You can’t bayesian your way out of a bad idea.
- Reasurring and has equipoise for ARF.
- Has challenged my assumptions for ACPO.
- I would still use NIV first line in COPD, and CPAP in ACPO.
- And what about yours…
Other resources
- Bottom line
- Ed and Todd Podcast
- Slides availible at doced.github.io